
Broadly NOFs can be categorised relative to the joint capsule into intracapsular or extracapsular.
Simply…
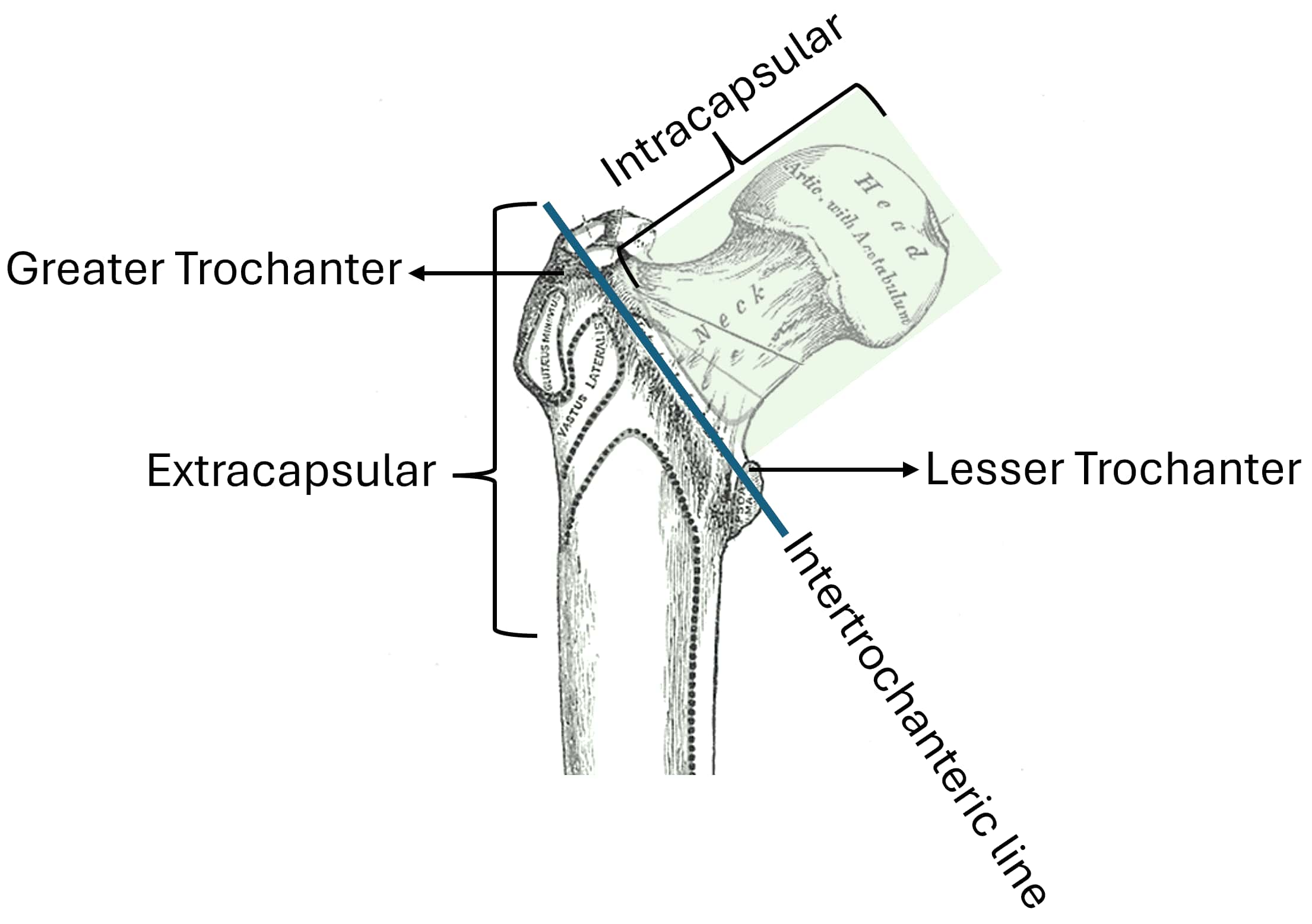
- Intracapsular being proximal to the intertrochanteric line.
- Extracapsular being distal to the intertrochanteric line.
Intracapsular can be further specified…
- Sub-capital (base of the head)
- Transcervical (across the neck)
- Basi-cervical (base of the neck)
Extracapsular is further sub-divided into…
- inter-trochanteric – between the greater and lesser trochanter.
- sub-trochanteric – distal to the lesser trochanter.
Extracapsular
- Intertrochanteric # – can be managed with dynamic hip screw (DHS) and plating, unless there is evidence of a reverse oblique fracture (3).
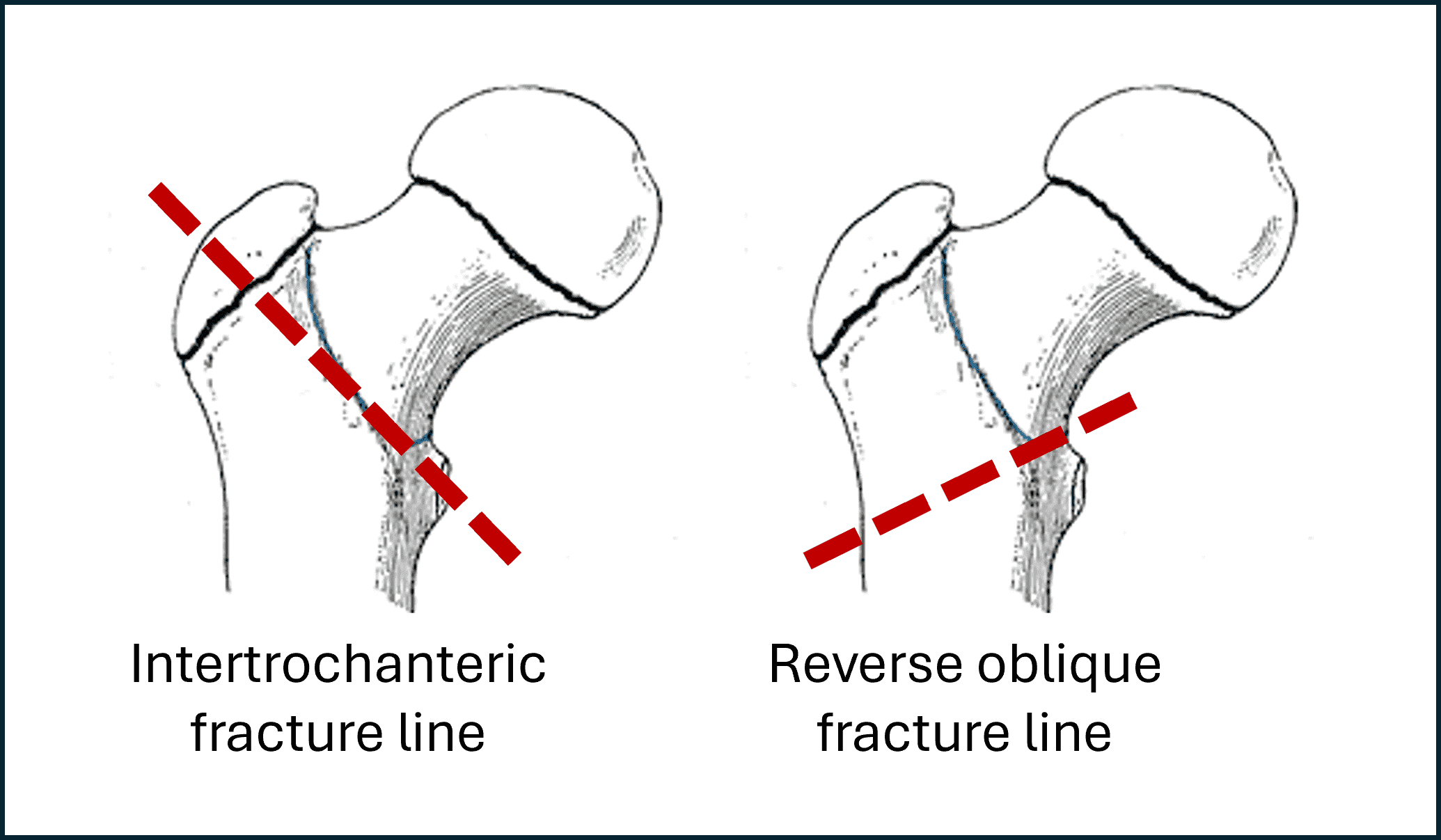
- Reverse oblique # – this is a more unstable fracture, it should not be seen as a classic intertrochanteric fracture, this is treated with an intermedullary (IM) nail.
Picture this fracture as almost a mirror image of an intertrochanteric fracture, where the fracture line extends from the medial cortex out through the lateral cortex.
- Sub-trochanteric # – this is a more unstable fracture, so a IM nail is often used to manage these fractures (3).