Distal Radial Fractures
Quick Links...
Background
Distal radial fractures are some of the most common fractures to be seen in the orthopaedic department. (1)
They occur in a bimodal presentation, peaking in the elderly population and in adolescents, with females more commonly affected in the older cohort and males more commonly affected in the younger cohort. (1)
High Yield Anatomy to Know…
- Bones of forearm and their features
- Carpal bones
- Median nerve course and innervations
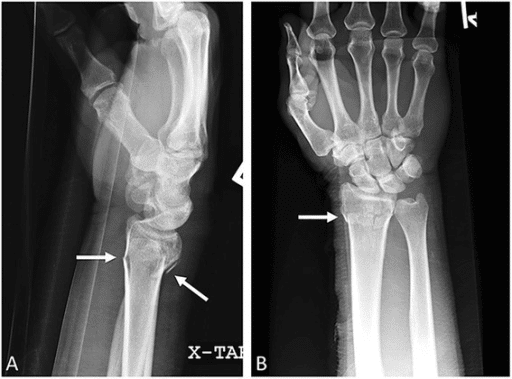
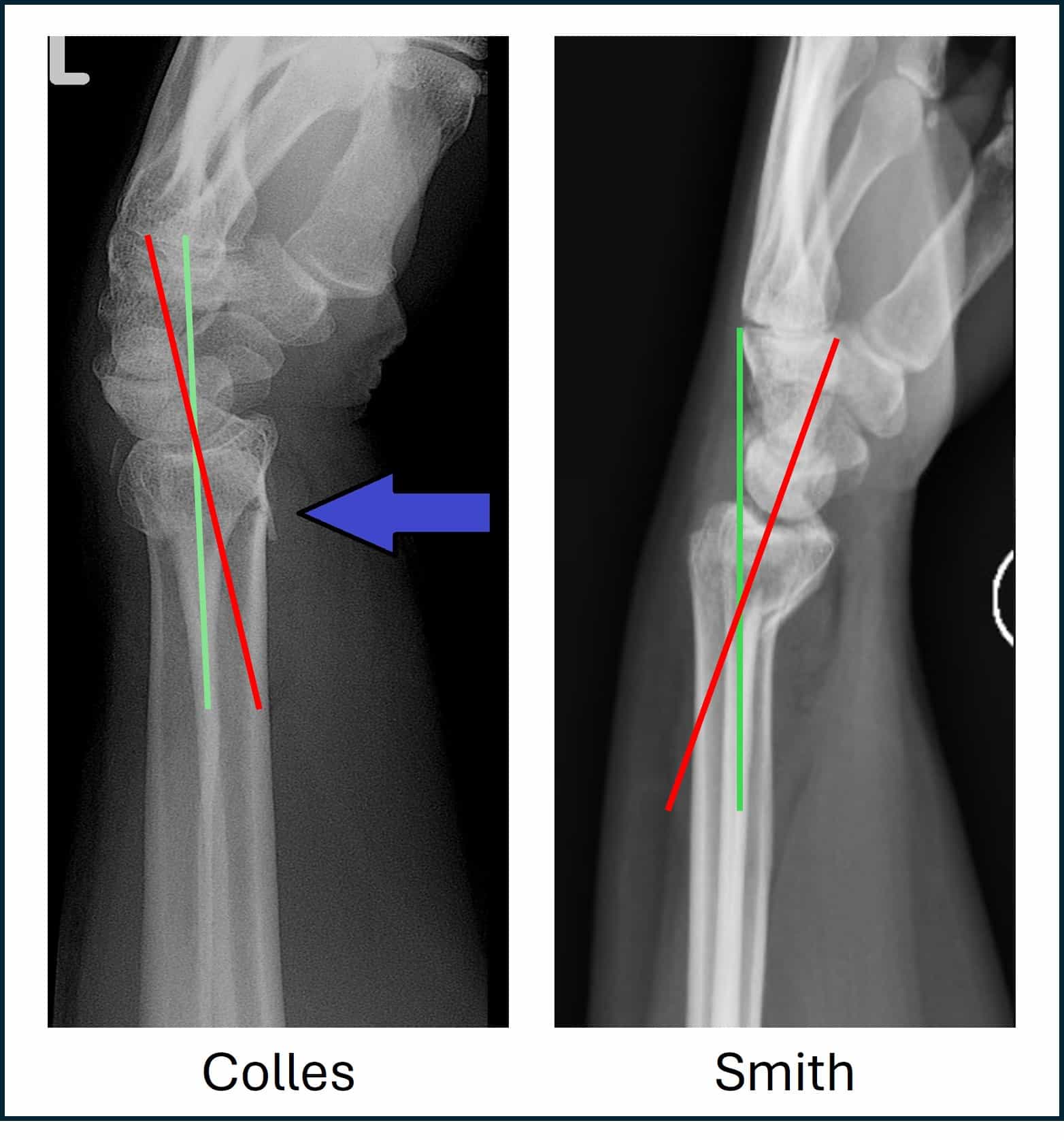
Types of Distal Radial Fractures
Colles – extraarticular with dorsal displacement and dorsal angulation, typically from fall onto extended wrist (Dinner Fork deformity).
Smith – extraarticular with volar displacement and volar angulation, typically from fall onto flexed wrist (Garden Spade deformity).
Barton – involves dorsal or volar intraarticular surface, often with radiocarpal dislocation/subluxation.
Chauffeur (aka Hutchinson fracture) – intraarticular fracture of the radial styloid process.
Die Punch – intraarticular impaction fracture of the lunate fossa.


Presentation
Most patients will describe a fall onto an outstretched hand (FOOSH).
Wrist pain, swelling, bruising, deformity.
Movement limited by pain.
Management
Initial…
- ABCDE
- Appropriate analgesia (2)
- oral paracetamol for mild pain
- oral paracetamol and codeine for moderate pain
- intravenous paracetamol supplemented with intravenous morphine titrated to effect for severe pain.
- Do not offer non-steroidal anti-inflammatory drugs (NSAIDs) to frail or older adults with fractures.
- Exclude compartment syndrome
- Assess median nerve sensation and motor (thenar weakness)
- Assess vascular status
- Skin condition?
- X-ray at least AP and lateral
- Assessment in Fracture Clinic within 72 hours (3)
- Social Hx – thinking discharge planning
- Any anticoagulation regular medication?
- Any other medications need to stop/change prior to surgery?
- Any polytrauma?
- Long lie? – ?rhabdomyolysis, check CK
- Other bloods: FBC, U&E, coag, group&save
- Does cause of fall need exploring? – ECG
- Bone health? – osteoporosis?
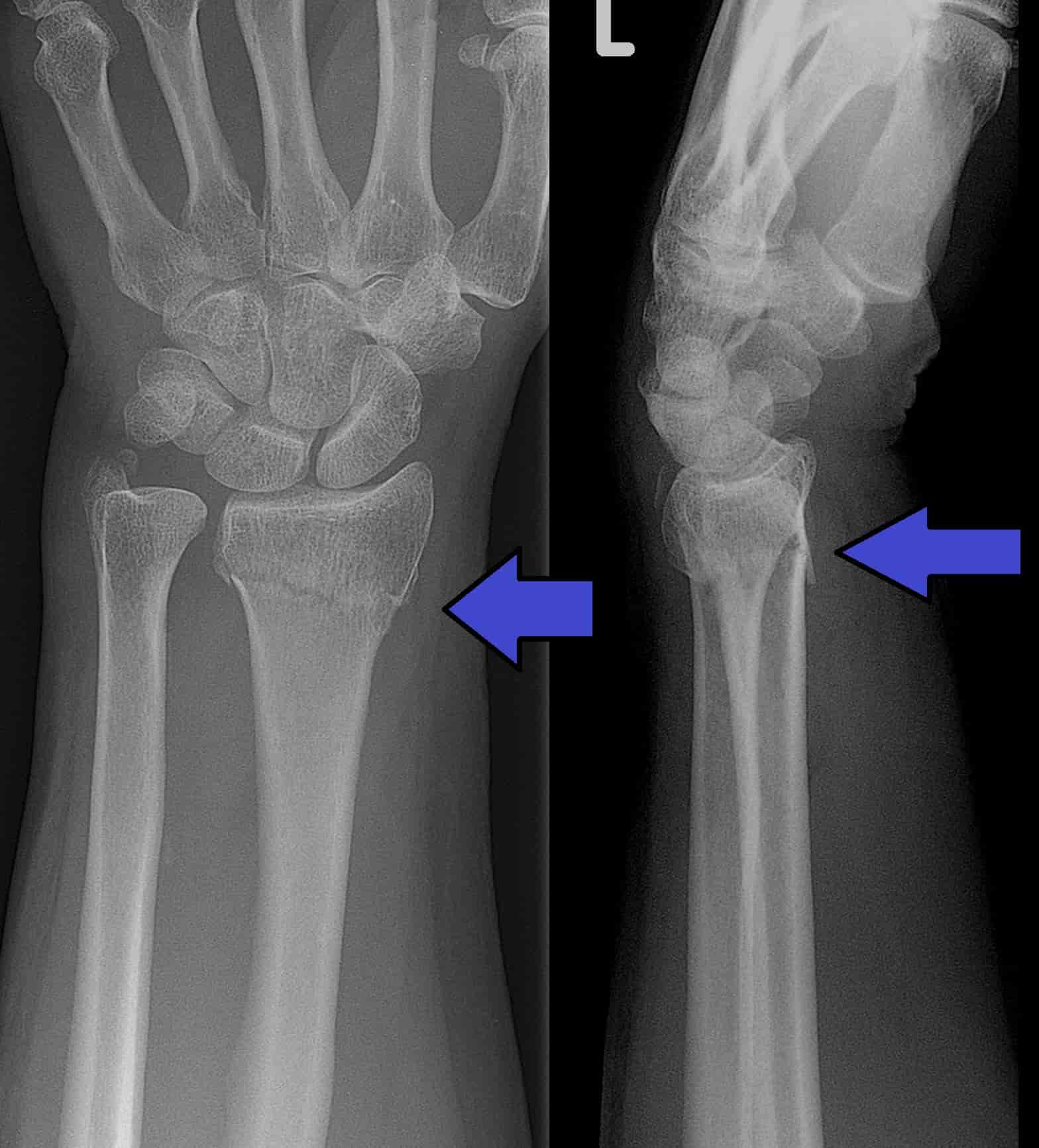
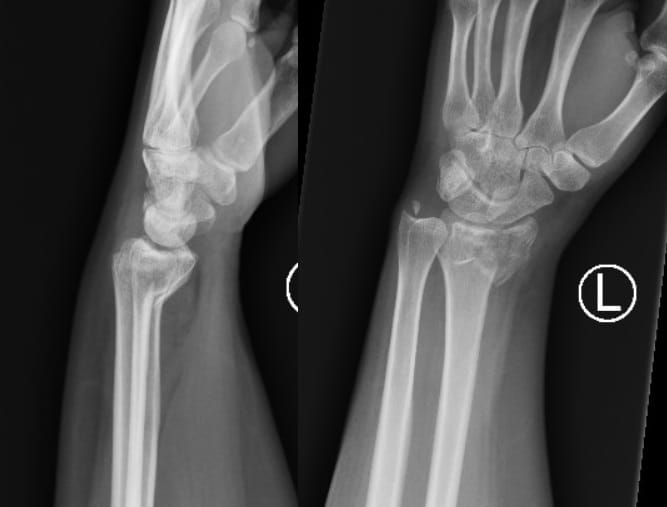
Imaging...
- X Rays: AP, lateral and oblique
- Comment on…
- Type of distal radial fracture?
- Any displacement?
- Any joint involvement?
- Associated Ulnar Styloid fracture?
See ‘The Orthopaedic X Ray’ for more information on fracture description/presentation.
Distal Radial Fracture Radiographic Criteria (4,5)
| Measurement | Radiograph required | Normal | Acceptable Limits | Post-Reduction Acceptable Limits |
|---|---|---|---|---|
| Radial Inclination | AP | ~23o | Change < 5o | |
| Radial Height | AP | ~13mm | <5mm shortening | <3mm shortening |
| Intra-articular Step | AP | Congruous | <2mm step | <2mm step |
| Angulation | Lateral | ~11o | Dorsal angulation <5o or <20o of contralateral side | Dorsal angulation <10o |
Features to assess on radiograph that indicate more severe fracture:
- Oblique, Spiral or Comminuted fracture
- Significant degree of angulation
- Intra-articular involvement
- Associated Ulna Styloid fracture
- Associated Scaphoid fracture
- Associated Radioulnar joint dislocation (Galeazzi fracture)
- Associated ligament injury – Scapholunate dissociation >3mm (Terry-Thomas sign)
Reduction of the Fracture...
- Consider IV regional block (Bier’s Block) when reducing in the ED, ‘Gas and Air’ is not suitable on its own for fracture reduction (2).
- Following reduction and immobilization with back slab plaster, re-image to assess reduction (see ‘Radiographic Criteria’).
Non-operative vs Operative Management
This is in fact an ongoing debate in the field of hand surgery, with some clinical trials – the DRAFFT Trials – indicating that there is no difference in patient outcomes between plastering, K-wire, or ORIF for a particular demographic of patients.
However, below are some common considerations made when deciding whether surgery is the right treatment option or not.
| Non-Operative Considerations (3,6,7) | Operative Considerations (3,6,7) |
|---|---|
| Extra-articular. | Intra-articular. |
| Within acceptable radiographic limits. | Beyond acceptable radiographic limits. |
| >65yrs with dorsally displaced fracture (Colles’) and absence of significant deformity or neurological compromise. | Volar displacement (volar displacement is more unstable). |
| Stable Fracture. | Unstable fracture. |
| Associated ulnar styloid fracture (ulnar styloid fracture does not require fixation, but may indicate more severe fracture (8)). | |
| Comminution. | |
| Die-punch fractures. | |
| Open fractures. | |
| Patient desire for earlier mobilisation. |
LaFontaine predictors of instability (9)
- radial shortening and dorsal comminution are the most predictive of instability
- severe osteoporosis, increased age
- associated ulnar fracture (weaker predictor)
- dorsal comminution > 50%, palmar comminution, intraarticular comminution
- dorsal angulation > 20°
- initial displacement > 1cm
- initial radial shortening > 5mm
Non-Surgical Treatment
- Below arm cast or splint.
- When casting, the wrist should be in neutral flexion, not forced palmer flexion (3).
- Repeat X-rays 2 weeks post injury/manipulation, where it is thought that the fracture is unstable AND if subsequent displacement is observed then it will change the management (3).
- Consider mobilisation out of cast/splint from 4-6 weeks post injury following repeat X-rays to assess adequate union.
Surgical Treatment Options
When surgery is required, it should be performed within…
- 72 hours of injury for intra-articular fractures (2)
- 7 days of injury for extra-articular fractures (2)
If fracture is dorsally displaced, but requires surgery, offer…
- K-wire fixation if…
- There is no intra-articular involvement OR
- Displacement of radial-carpel joint can be reduced under closed manipulation (2).
- Open reduction and internal fixation (ORIF) if…
- Reduction of the joint surface is not possible under closed manipulation (2).
Children (skeletally immature)
Children with dorsally displaced fractures (including fractures involving a growth plate) who have undergone manipulation, consider…
- a below-elbow plaster cast OR (2)
- K-wire fixation if the fracture is completely displaced (2)
Guidelines
Fractures (non-complex): assessment and management
NICE guideline [NG38]Published: 17 February 2016
https://www.nice.org.uk/guidance/ng38/chapter/Recommendations
Management of Distal Radius Fractures
British Society for Surgery of the Hand (2018)
https://www.bssh.ac.uk/professionals/management_of_distal_radial_fractures.aspx
BOAST – The Management of Distal Radial Fractures (2017)
https://www.boa.ac.uk/resource/boast-16-pdf.html
BOAST – Early Management of the Paediatric Forearm Fracture (2021).
https://www.boa.ac.uk/resource/boast-early-management-of-the-paediatric-forearm-fracture.html
References
- Davis ES, Chung KC. Chapter 2 – Epidemiology of Distal Radius Fractures. In: Jupiter J, Chammas M, editors. Distal Radius Fractures [Internet]. Elsevier; 2021 [cited 2024 Apr 19]. p. 13–9. Available from: https://www.sciencedirect.com/science/article/pii/B9780323757645000342
- Recommendations | Fractures (non-complex): assessment and management | Guidance | NICE [Internet]. NICE; 2016 [cited 2024 Apr 19]. Available from: https://www.nice.org.uk/guidance/ng38/chapter/Recommendations#management-in-the-emergency-department
- BOA. BOAST – The Management of Distal Radial Fractures [Internet]. [cited 2024 Apr 19]. Available from: https://www.boa.ac.uk/resource/boast-16-pdf.html
- Mulders M, Rikli D, Goslings J, Schep N. Classification and treatment of distal radius fractures: a survey among orthopaedic trauma surgeons and residents: European Journal of Trauma & Emergency Surgery. EUR J TRAUMA EMERG SURG. 2017 Apr;43(2):239–48.
- Lichtman DM, Bindra RR, Boyer MI, Putnam MD, Ring D, Slutsky DJ, et al. Treatment of Distal Radius Fractures. JAAOS – Journal of the American Academy of Orthopaedic Surgeons. 2010 Mar;18(3):180.
- Ju JH, Jin GZ, Li GX, Hu HY, Hou RX. Comparison of treatment outcomes between nonsurgical and surgical treatment of distal radius fracture in elderly: a systematic review and meta-analysis. Langenbecks Arch Surg. 2015 Oct;400(7):767–79.
- Saka N, Zenke Y. Chapter 8 – Surgical Versus Conservative Interventions for Displaced Distal Radius Fractures. In: Jupiter J, Chammas M, editors. Distal Radius Fractures [Internet]. Elsevier; 2021 [cited 2024 Apr 19]. p. 69–83. Available from: https://www.sciencedirect.com/science/article/pii/B9780323757645000160
- Kim JK, Koh YD, Do NH. Should an ulnar styloid fracture be fixed following volar plate fixation of a distal radial fracture? J Bone Joint Surg Am. 2010 Jan;92(1):1–6.
- Walenkamp MMJ, Aydin S, Mulders MAM, Goslings JC, Schep NWL. Predictors of unstable distal radius fractures: a systematic review and meta-analysis. J Hand Surg Eur Vol. 2016 Jun 1;41(5):501–15.