Galeazzi vs Monteggia
Many people may confuse these eponymous names with the respective similar fracture-dislocation presentation.
Therefore, the following aide memoir may be of use during this learning process…
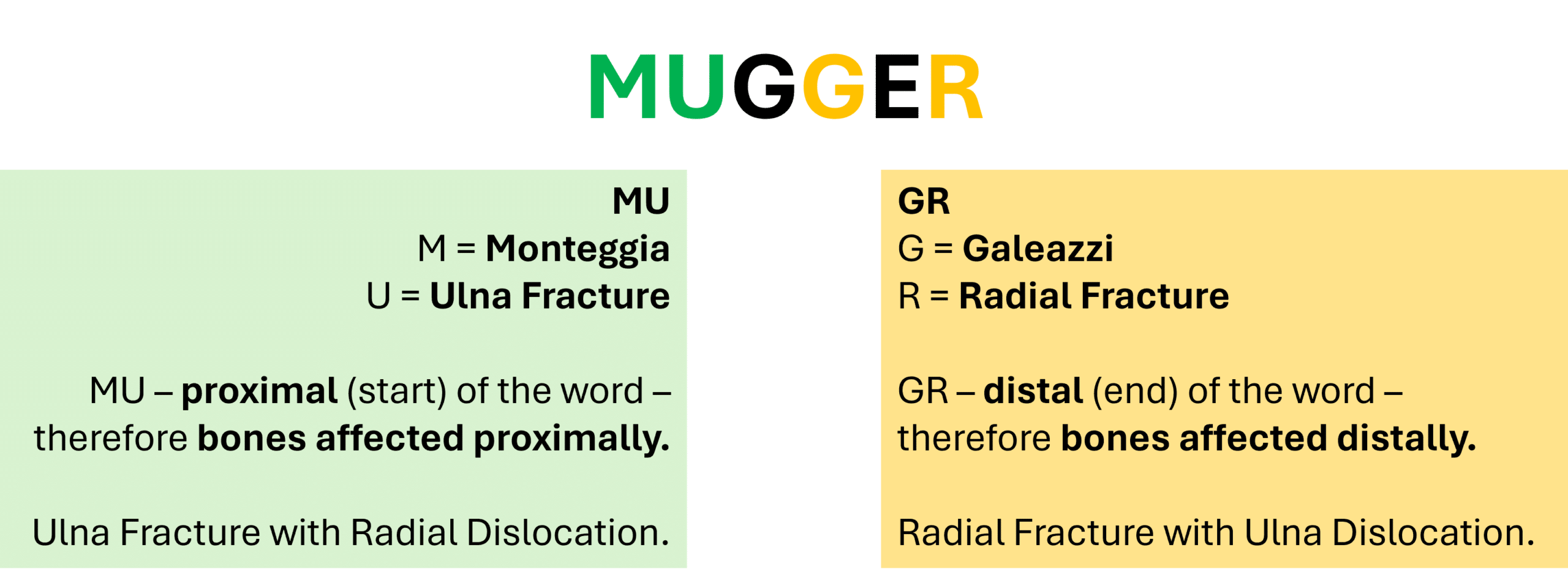
Just remember the word ‘Mugger’ and that the aide memoir only refers to the fracture – so you just need to remember the other bone (not the fractured bone) is dislocated.

- X Ray: AP, Lateral, Oblique of Forearm, Elbow, Wrist
- Comment on…
- Radial fracture…
- Location
- Angulation
- Degree of Shortening
- Unla subluxation…
- Direction
- Radial fracture…
See ‘The Orthopaedic X Ray’ for more information on fracture description/presentation.