Scaphoid Fractures
Quick Links...
Background
Scaphoid Fractures are the most common carpel fracture and account for 15% of all acute wrist fractures (1).
They predominantly affect young males. They are more uncommon in the paediatric or elderly population as the distal radius tends to fracture first (1,2).
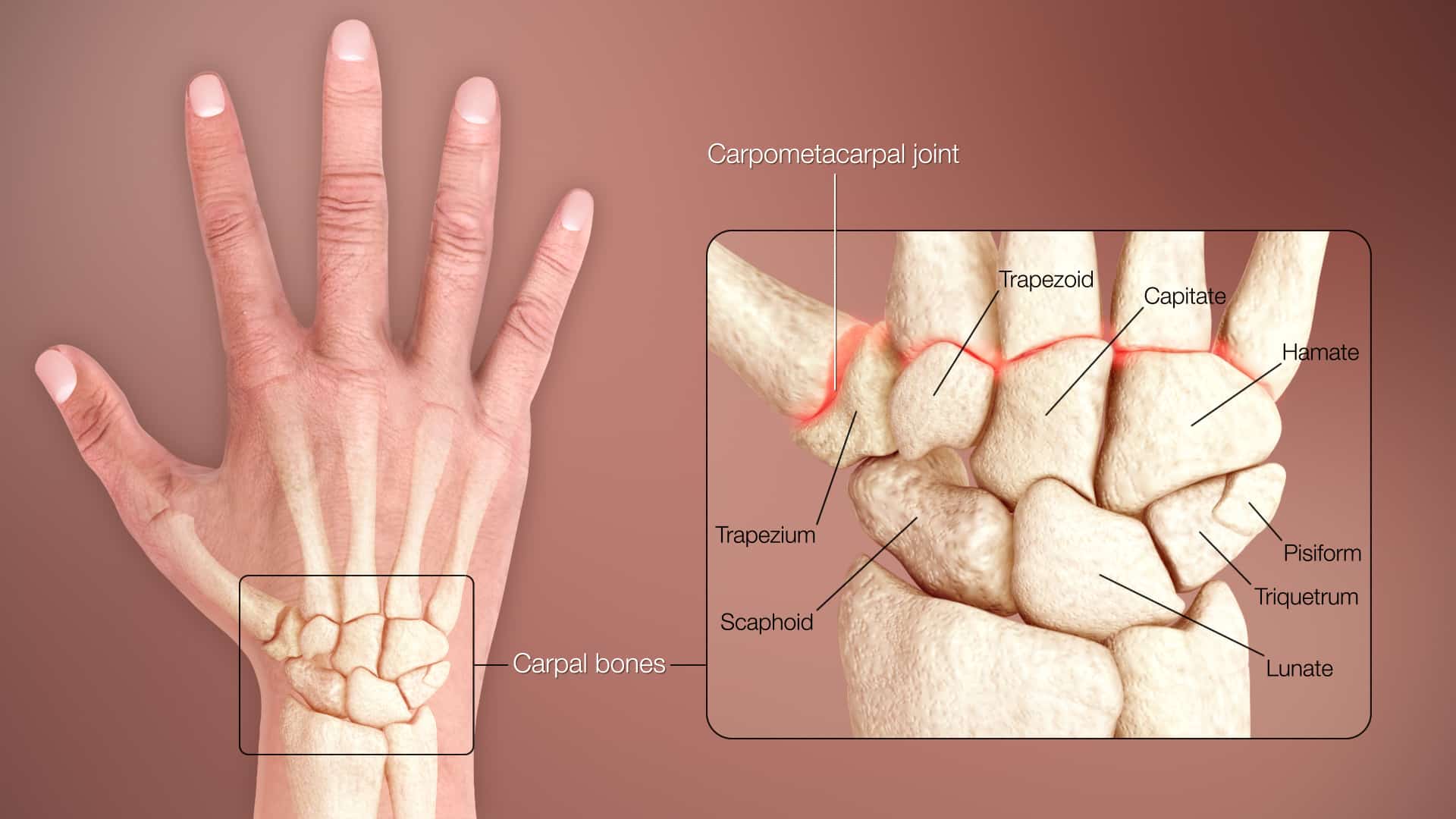
High Yield Anatomy to Know…
- Carpal bones (scaphoid links the proximal and distal row)
- Blood supply to the Scaphoid bone
Presentation
Patients classically present with a fall onto an outstretched hand (FOOSH).
May be some wrist swelling.
Pain with circumduction of the wrist.
Specific tests:
- Anatomical snuffbox tenderness
- Scaphoid tubercle tenderness
- Positive scaphoid compression test (pain with axial loading of thumb metacarpal)
Management
Initial…
- ABCDE
- Appropriate analgesia (3)
- oral paracetamol for mild pain
- oral paracetamol and codeine for moderate pain
- intravenous paracetamol supplemented with intravenous morphine titrated to effect for severe pain.
- Do not offer non-steroidal anti-inflammatory drugs (NSAIDs) to frail or older adults with fractures.
- Exclude compartment syndrome
- Assess neurovascular status
- Skin condition?
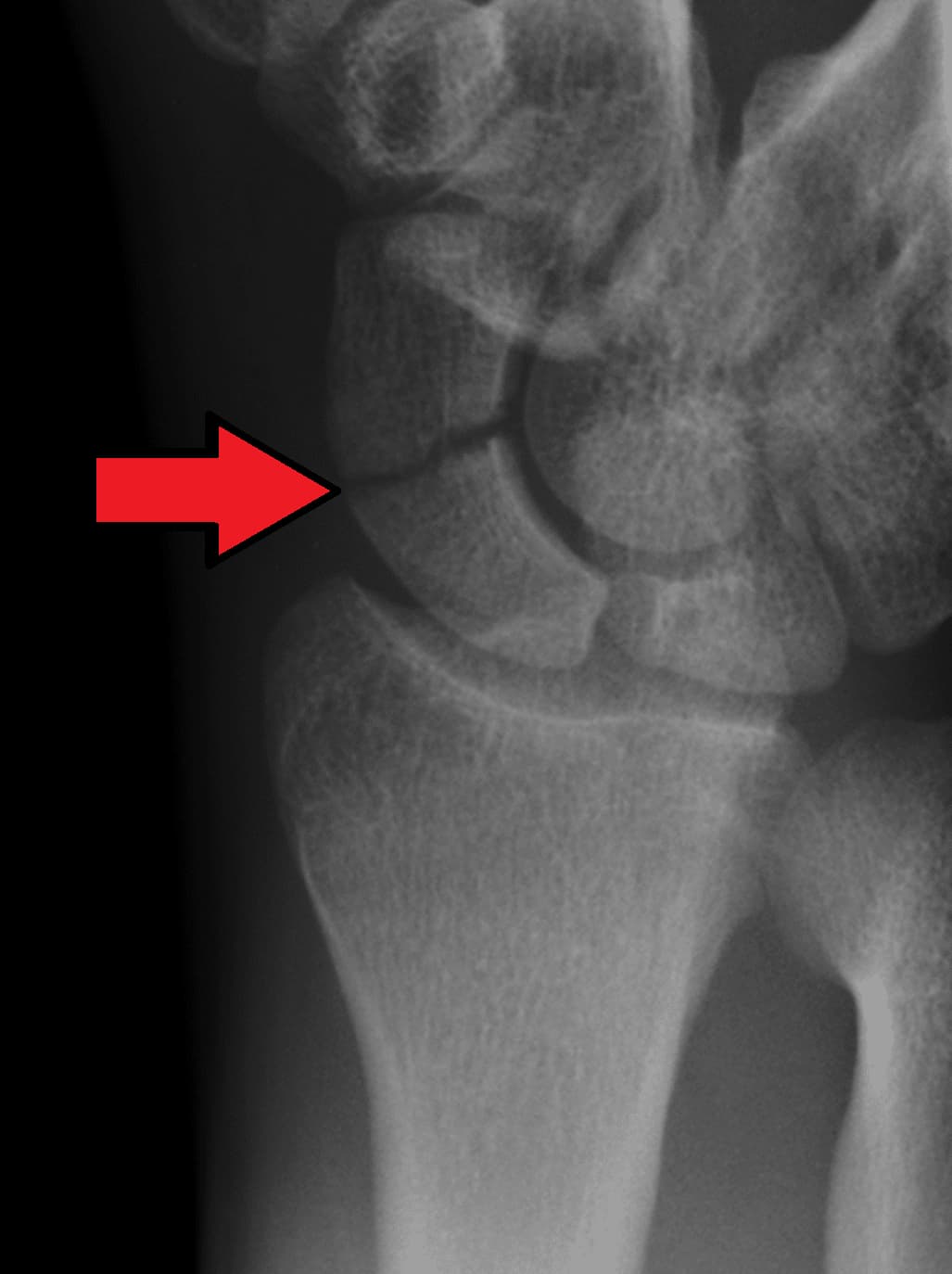
Imaging
- X-ray at least AP and lateral
- Consider MRI as first line for suspected scaphoid fractures following thorough clinical examination (3).
- CT scans are also often used to help further visualise the fracture and are recommended by the BSSH pathway (see (4)).
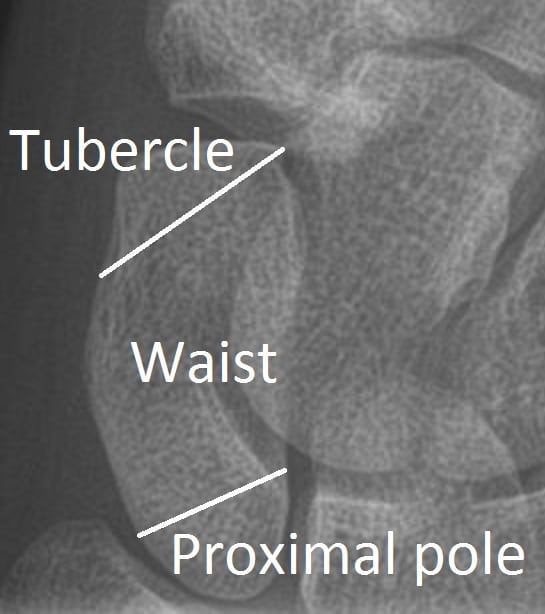
- Important to note:
- Location of fracture (distal pole, waist, proximal pole)
- Any displacement
- Any articular surface involvement
If X-ray are negative for any fracture, but there is high clinical suspicion, then the wrist should be immobilised with splint or cast with repeat x-rays arranged in 7-14 days’ time (1).

Treatment Options
Non-operative…
Cast immobilisation.
Indications:
- Non-displaced stable fracture (particularly of the distal pole)(5).
Operative (4) …
Percutaneous screw
Indications:
- Proximal pole fractures (6)
- Displacement >2mm (7)
- Non-displaced fracture of waist if patient requiring faster return of mobility.
Open Reduction and Internal Fixation (ORIF)
Indications(1):
- Significantly displaced fractures
- Associated peri-lunate dislocation
- Comminuted fractures
- Unstable vertical or oblique fractures
Complications
- Non-union is the main complication with this fracture.
- This is more common with proximal pole fractures.
- Non-union should be treated promptly (7), often with ORIF and bone graft.
- Avascular necrosis (AVN) and is another complication of this fracture.
- Again, this complication is more common with proximal pole fracture.
Guidelines
Fractures (non-complex): assessment and management
NICE guideline [NG38]Published: 17 February 2016
https://www.nice.org.uk/guidance/ng38/chapter/Recommendations
Management of Scaphoid Fractures (4)
BSSH Guidelines: [cited Apr 2024]
https://www.bssh.ac.uk/professionals/guidelines.aspx
https://www.bssh.ac.uk/_userfiles/pages/files/professionals/girft/girft-scaphoid.pdf
References
- Hayat Z, Varacallo M. Scaphoid Wrist Fracture. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Apr 27]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK536907/
- Dias J, Brealey S, Choudhary S, Cook L, Costa M, Fairhurst C, et al. Scaphoid Waist Internal Fixation for Fractures Trial (SWIFFT) protocol: a pragmatic multi-centre randomised controlled trial of cast treatment versus surgical fixation for the treatment of bi-cortical, minimally displaced fractures of the scaphoid waist in adults. BMC Musculoskelet Disord. 2016 Jun 4;17:248.
- Recommendations | Fractures (non-complex): assessment and management | Guidance | NICE [Internet]. NICE; 2016 [cited 2024 Apr 19]. Available from: https://www.nice.org.uk/guidance/ng38/chapter/Recommendations#management-in-the-emergency-department
- Guidelines | The British Society for Surgery of the Hand [Internet]. [cited 2024 Apr 27]. Available from: https://www.bssh.ac.uk/professionals/guidelines.aspx
- Dias JJ, Wildin CJ, Bhowal B, Thompson JR. Should acute scaphoid fractures be fixed? A randomized controlled trial. J Bone Joint Surg Am. 2005 Oct;87(10):2160–8.
- Grewal R, Lutz K, MacDermid JC, Suh N. Proximal Pole Scaphoid Fractures: A Computed Tomographic Assessment of Outcomes. J Hand Surg Am. 2016 Jan;41(1):54–8.
- Dias JJ, Brealey SD, Fairhurst C, Amirfeyz R, Bhowal B, Blewitt N, et al. Surgery versus cast immobilisation for adults with a bicortical fracture of the scaphoid waist (SWIFFT): a pragmatic, multicentre, open-label, randomised superiority trial. Lancet. 2020 Aug 8;396(10248):390–401.