Galeazzi vs Monteggia
Many people may confuse these eponymous names with the respective similar fracture-dislocation presentation.
Therefore, the following aide memoir may be of use during this learning process…
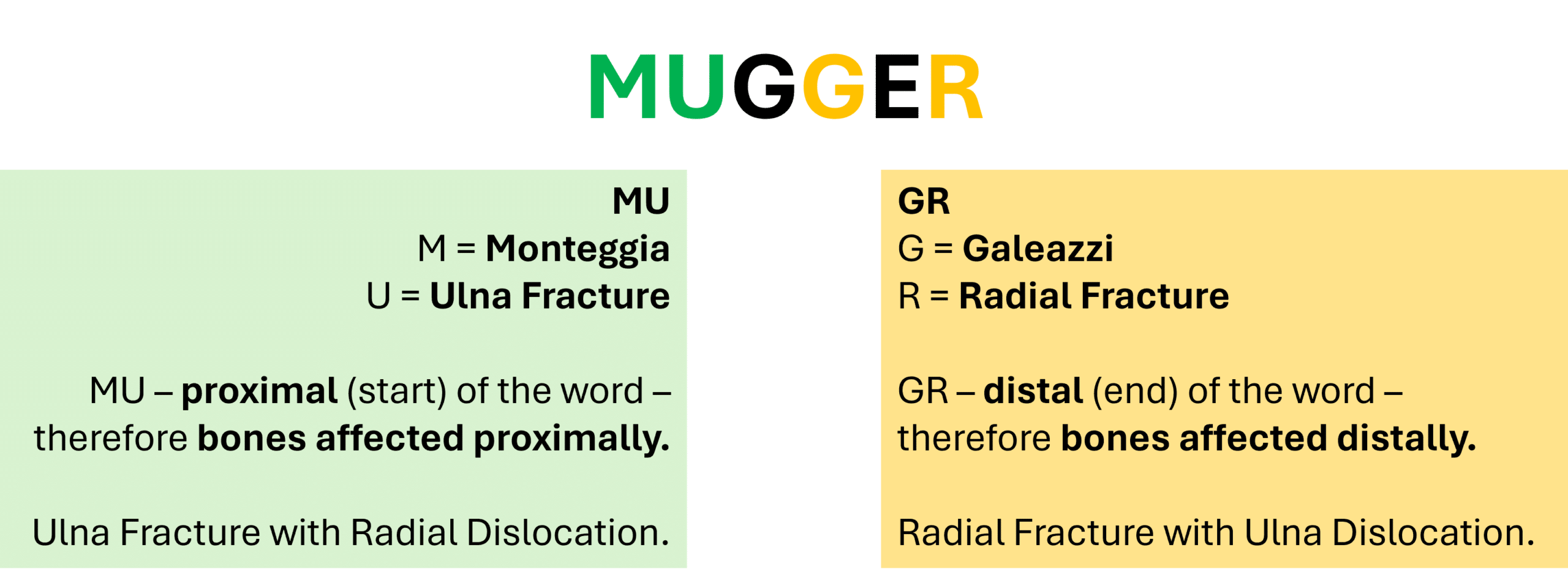
Just remember the word ‘Mugger’ and that the aide memoir only refers to the fracture – so you just need to remember the other bone (not the fractured bone) is dislocated.
Monteggia fractures are often classified according to the Bado Classification (2).
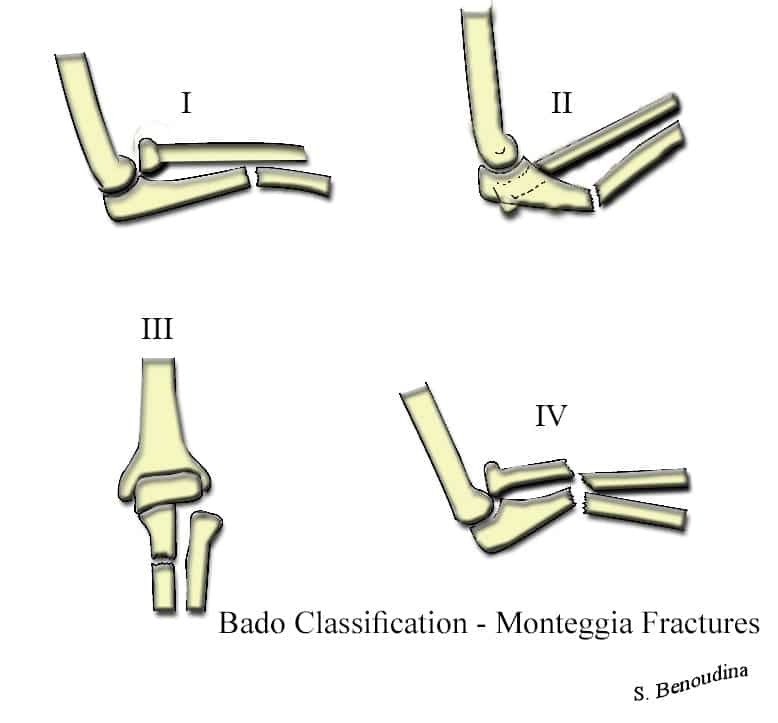
The Bado Classification categorises these fractures into 4 types…
- Type I – anteriorly angulated ulna fracture with anterior dislocation of radial head.
- Type II – posteriorly angulated ulna fracture with posterior dislocation of radial head.
- Type III – laterally angulated fracture of ulna metaphysis with lateral radial head dislocation.
- Type IV – Proximal fracture of both ulna and radius.

- X Ray: AP, Lateral, Oblique of Forearm, Elbow, Wrist
- Comment on…
- Pt Age (important to consider degree of bone ossification at the elbow if skeletally immature)
- Any concomitant distal radial fracture?
- Consider CT scan if involvement of coronoid, olecranon, radial head fracture.
See ‘The Orthopaedic X Ray’ for more information on fracture description/presentation.